+1(209) 348-9544
order@myessayservices.com
+1(209) 348-9544
order@myessayservices.com
![]() Are you in High School, College, Masters, Bachelors or Ph.D and need someone to help write your paper? All you need is to ask for research paper help written by a specialist in your academic field. When you buy an essay online from us, we offer you an original, nil plagiarized and unique paper written by a dedicated writer who is PhD or Masters qualified. MyEssayServices.com is an experienced service with over 9 years experience having delivered over 83,000 essays over the years.
Are you in High School, College, Masters, Bachelors or Ph.D and need someone to help write your paper? All you need is to ask for research paper help written by a specialist in your academic field. When you buy an essay online from us, we offer you an original, nil plagiarized and unique paper written by a dedicated writer who is PhD or Masters qualified. MyEssayServices.com is an experienced service with over 9 years experience having delivered over 83,000 essays over the years.

 United States is located in the continent of North America. The country has an approximate population of 318 million people. The health indicators for the country entail life expectancy, the probability of children dying at the under the age of five and that from 15-60 years per 1000. The total amount of money country spends on health per capita, and the expenditure on health as a percentage of the GDP are examined (WHO, 2013). The country records a life expectancy of 76 years for the males and 81 for females. Ladies within the age set of 15-60 records the lowest death rate of 77 out of 1000 while males the highest of 130.
United States is located in the continent of North America. The country has an approximate population of 318 million people. The health indicators for the country entail life expectancy, the probability of children dying at the under the age of five and that from 15-60 years per 1000. The total amount of money country spends on health per capita, and the expenditure on health as a percentage of the GDP are examined (WHO, 2013). The country records a life expectancy of 76 years for the males and 81 for females. Ladies within the age set of 15-60 records the lowest death rate of 77 out of 1000 while males the highest of 130.
The country spends a total of 17.9 percent of its GDP on health with the expenditure per capita translating to 8608 million dollars (Mathers, 1999). It has the lowest child mortality of children under the age of five being seven out of 1000 people. In contrast, Dominican Republic has a population of 10.277 million people. A thorough examination of the health indicators shows that the life expectancy for male is 76 years while that of females is 78 years. The child mortality records 27 out of 1000 live births when the children attain the age of five years.
The probability of male dying when they attain the age of between 15-60 years is 137 while for female is 93(WHO, 2013). In comparison to the U.S, the country spends 529 million dollars as the total expenditure per capita on health. Dominican Republic has a lower percentage expenditure on health recording 5.4%. U.S uses approximately 17.9 percent of its GDP on the health while Dominican Republic spends 5.4 percent. The American figure represents 3 times that of Dominican Republic.
The demographics of the United States is very high comparing to that of Dominican Republic thus, the country has to spend more of its GDP in health. Perhaps because of better health facilities and other factors, U.S has a lower child mortality rate of 7 in comparison to that of Dominican Republic that record 27 out of 1000 babies (WHO, 2013). The life expectancy for the both countries stand almost at the same point with that of the U.S for males being 76 and that of females being 81.
The Dominican Republic expectancy are 76 and 78 m/f respectively. The average life expectancy for the United States is 78.5 while that for Dominican Republic standing at 77. This is quite shocking given the difference in spending of the two countries yet having almost equal life expectancy levels. Other health indicators indeed differ between the two with a large margin, but life expectancy being approximately equal (Mathers, 1999).
In comparison to the past, great strides have been made in the area of health indicators. There has been a decrease in life expectancy at birth (Mather, 2001). The life expectancy decrease could be attributed to an increase in the death rate arising from coronary heart disease and stroke. Richmond, CA still faces challenges in public health with significant high percentage of health disparities. Life expectancy at Richmond could be on the decline because of increased cases of obesity (McCoy, 2006). Obesity as a risk factor contributes to health related problem such as Coronary Heart disease and diabetes. These are some of the chronic illness that contribute to a reduction in the life expectancy.
Furthermore, life expectancy has been reduced as a result of increased asthma hospitalization especially among the youths (Corburn, 2013). Richmond community among others shows stagnating life expectancy while the overall longevity of the national expectancy level has been increasing upward. There is a high probability that girls born may live shorter lives in comparison to their mothers. Life expectancy at Richmond is 12 years less with the mean having 66.9 years a figure that record the lowest life expectancy when comparing to other cities within the U.S. Although a significant increase in life expectancy from the lowest of 61.7 years on average. The average life expectancy at the national level stands at 78.9.
The rising levels of obesity and smoking are prime reasons behind the decrease in life expectancy. Other potential reasons include the increase in the cases of chronic illnesses affecting the community. The morbidity at mortality rate of the Richmond Community is high due to a reduction in the life expectancy among the populations. Child mortality also stands at its highest recording a shocking value of 10 in 1000 live births while the natural level remaining at 7. This indicates an increment of three more child deaths in Richmond (Corburn, 2013).
There are associated risk factors that lead to diseases that contribute to increasing mortality and morbidity rates. People have contracted chronic illnesses that do no good other than decreasing their life expectancy level. Health disparities are still common in the Community with people in the neighborhood having little money to spend in acquisition of necessary medical attention. Most are incapable of raising the money required for procedures such as kidney dialysis. The patients and their families opt for home care that is insufficient in the management of the diseases (Corburn, 2013).
References
Corburn, J. (2013). Healthy city planning: From neighbourhood to national health equity. New York: Routledge
Mathers, C.D. (1999, May-June). Gains in health expectancy from the elimination of diseases among older people. Disability And Rehabilitation, 21(5-6), 211–221. PMID: 10381233.
Mathers, C.D. (2001, May 26). Healthy life expectancy in 191 countries, 1999. Lancet, 357(9269), 1685–1691. PMID: 11425392.
McCoy, D.C. (2006, April). Translating words into actions: Are governments acting on the advice of the World Health Report? Bulletin of The World Health Organization, 84(4), 327–331. PMID: 16628307.
WHO (2013, March 29). WHO | Countries.
The right sided heart failure is caused by the failure of the right side of the heart. The right ventricle fails to supply adequate blood to the lungs. The right sided heart failure occurs in about one person in every twenty people. The result is that the blood supposed to go to the lungs flows to other body parts leading to congestion. The most affected parts of the body by this congestion include the liver, limbs and the gastrointestinal tracts (Porth, 2011). One of the main causes of the right sided heart failure is the failure of the left side of the heart. This puts so much pressure on the right side leading to possible failure. Some of the classical signs of the right sided failure include pulmonary edema, heart failure, congenital heart disease, and the chronic disease of the muscle of the heart.
Some of the disorders that result in the right sided heart failure are the same classical signs. One of them is hypertension which is the abnormality of the blood pressure. Cardiomyopathy is a chronic disease that affects the muscles of the heart and is a result of the failure of the muscles of the right ventricle. Pulmonary edema leads to the shortness of breath due to the buildup of fluids in the air sacs in the lungs. Another disorder that results from the failure of the right ventricle is the heart valve disease (Lilly, 2011).
The left sided heart failure, on the other hand, is a failure of the left ventricle to supply blood to body parts. This condition is more common than the right sided heart failure, and it is a life threatening condition. In this case, the left ventricle fails to supply enough oxygenated blood to the body parts. The patient experiences fatigue during exercise or ant activity. This is because the body is in the lack of oxygenated blood. The patient may also experience shortness in breathe or pulmonary edema due to the accumulation of fluids in the lungs. The common causes of the left side heart failure include heart failure and high blood pressure.
The excessive consumption of alcohol also puts one at the risk of being exposed to the failure of the left ventricle. There is a couple of disorders that result from the left sided heart failure, and they happen to be the same as those of the right sided failure. Any disease that may result in the damage of the heart is very common with the left sided failure (Porth, 2009). Other common disorders that results include the narrowing of valves, hypothyroidism, infection of the heart muscles, and the blockages of the heart arteries. In every three people out of a hundred people, one person is prone to the left sided heart failure.
References
Lilly, L. S., & Harvard Medical School. (2011). Pathophysiology of heart disease: A collaborative project of medical students and faculty. Baltimore, MD: Wolters Kluwer/Lippincott Williams & Wilkins.
Porth, C., & Porth, C. (2011). Essentials of pathophysiology: Concepts of altered health states. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins.
Porth, C., Matfin, G., & Porth, C. (2009). Pathophysiology: Concepts of altered health states. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins.
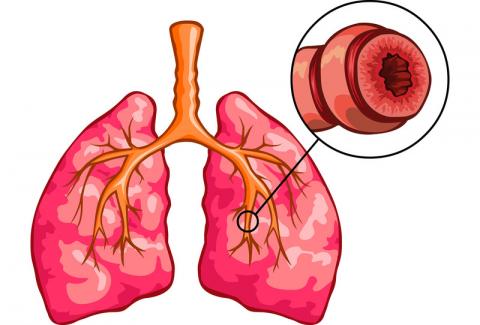 Asthma is an infection that affects the lungs causing an inflammation and the blocking of the airway. It causes often wheezing periods, coughing mostly happens during the night, and early mornings, chest tightness and one may run short of breath at times. Asthma starts mostly at childhood though it is an all age disease. Inhaled corticosteroids are used for the long-term control of asthma. The corticosteroids are used to reduce the inflammation caused by the mucus in the airways which is located in the bronchial tubes. The inhaled corticosteroids have proven to be effective when it comes to the treatment of persistent asthma (Ellis, 1998). The reduction in the inflammation in the airways helps reduce the chances asthma attacks.
Asthma is an infection that affects the lungs causing an inflammation and the blocking of the airway. It causes often wheezing periods, coughing mostly happens during the night, and early mornings, chest tightness and one may run short of breath at times. Asthma starts mostly at childhood though it is an all age disease. Inhaled corticosteroids are used for the long-term control of asthma. The corticosteroids are used to reduce the inflammation caused by the mucus in the airways which is located in the bronchial tubes. The inhaled corticosteroids have proven to be effective when it comes to the treatment of persistent asthma (Ellis, 1998). The reduction in the inflammation in the airways helps reduce the chances asthma attacks.
The two common types of medication for asthma are Proair and Pulmicort. The use of these inhalers comes with some safety precautions which every patient is expected to follow. One of them includes that the inhalers can be used every 4-6 hour. The inhalers can also be used, before any exercises, to avoid the patient running out of breath. The main disadvantage of the use of inhaled corticosteroids is that there are side effects. The patient must also shake the inhaler five to six times before using the inhaler (Gedatus, 2000). These side effects include sore throat, fungus infection in the mouth, and delayed growth in children, headache, dizziness and high blood pressure.
Patients are advised to follow some procedures to reduce the risk of being prone to the side effects. The most common one being that one should rinse their mouth before using the inhaler. Doctors also advice on the use of a spacer rather than an inhaler. This is because a spacer can deliver medicine to the lungs better than an inhaler. A peak flow meter is a device that is used to measure how good a patient’s asthma is under control. This is done be measuring the air that flowing out of the lungs, and the patient is expected to blow into the device. The device can detect when to stop or the progress of the medication, what causes the attacks or when one should seek medical care.
Laryngotracheobronchitis, also known as croup, is an infection that affects mostly infants and children. The disease leads to difficulty in breathing and the production of a barking kind of cough. This is due to a viral infection in the upper airway which causes the throat to sweat. For the disease, hospitalization is very rare though the cough is more persistent at night. The use of epinephrine or other steroids is the most commonly used treatment (Hess, 2012). Epiglottitis, on the other hand, is a disease caused by the infection of the epiglottis. The infection is uncommon in the recent times but is life threatening. The infection is mostly detected by high fever or sore throat. The other common symptoms include drooling, difficulty when breathing and swallowing, shaking and the production of some abnormal sounds when breathing.
Bronchiolitis is very common infection of the respiratory tract in younger children. In its early stages, the early symptoms are similar to those of common cold: a cough and a runny nose. The other symptoms later show up, and they include fever, difficulty when eating and the cough become persistent (Porth, 2009). In most cases, children who have Bronchiolitis tend to have asthma later on in their life. For a patient to possess typical signs and symptoms of acute respiratory distress there, is a history which is usually common. Some of the factors include premature birth, young age, and anatomic abnormalities (Smith, 2008). There are also other common symptoms which include cough or a history of stroke or seizure. All the above infections can cause acute respiratory distress.
References
Ellis, M. E. (1998). Infectious diseases of the respiratory tract. Cambridge: Cambridge University Press.
Gedatus, G. M., & Dolan, C. (2000). Mononucleosis. Mankato, Minn: LifeMatters.
Hess, D. (2012). Respiratory care: Principles and practice. Sudbury, Mass: Jones & Bartlett Learning.
Porth, C.M., & Matfin, G. (2009) Pathophysiology: Concepts of altered health states. (Eight ed.) Philadelphia, PA: Lippincott Williams & Wilkins.
Smith, T. L. (2008). Asthma. New York: Chelsea House Publishers.
Discussion question #1
 Within the past few years, asthma condition remains to be a high concern to public health in United States (Hamid, 2005). Asthma is a health condition that affects the respiratory system of the patient. It causes an inflammatory response on the bronchus of the patient (Porth, 2009). External stimuli such as temperature change, pollens and as well, smoke are responsible for triggering the response (Rush, 2007). Several deaths in United States are arising due to the condition. Medical researchers are using both external and environmental factors in explaining the increase in asthma prevalence (Smith, 2008).
Within the past few years, asthma condition remains to be a high concern to public health in United States (Hamid, 2005). Asthma is a health condition that affects the respiratory system of the patient. It causes an inflammatory response on the bronchus of the patient (Porth, 2009). External stimuli such as temperature change, pollens and as well, smoke are responsible for triggering the response (Rush, 2007). Several deaths in United States are arising due to the condition. Medical researchers are using both external and environmental factors in explaining the increase in asthma prevalence (Smith, 2008).
Initially, asthma treatment of asthma was by short-acting beta. This treatment involved control of chronic symptoms of asthma (Rush, 2007). Control of asthma immediate symptoms is by quick-relief medicine. The prescription on a patient prevents the exercise-induced asthma. Drugs used in dealing with the immediate symptoms of asthma include short-acting beta agonists and as well anticholinergic. Quick relief treatment of asthma aims at speeding up the recovery of the patient from exacerbations (Porth, 2009).
Over the past few years, there have been a change on the drugs used in treating asthma. Corticosteroids, often known as steroids, are anti-inflammatory medicine prescribed for patients suffering from asthma (Hamid, 2005). These drugs are effective while treating long-term asthma. There is a requirement by the doctor that the patient takes the drug on a daily basis (Porth, 2009). The drugs play a great role in keeping asthma under control and prevent cases of asthma attacks in the future. In United States, there have been a rise in the use of these steroids. This is due to their ability to prevent the production of chemicals responsible for causing inflammation. This on the other hand, prevents cases of tissue damage therefore an effective way of dealing with long-term asthma cases (Smith, 2008).
Discussion Question #2
Laryngotracheobronchitis (croup) is a health disorder that affects the larynx, trachea and the bronchus of the patient. This condition is common among children between the age of 3 months and 5 years. As a respiratory disorder, it has its distinctive symptom as wet breaking cough. In addition, the patient displays stridor sounds during auscultating of the lungs (Smith, 2008).
On the other hand, epiglottitis is a respiratory condition mostly seen in children between the ages below seven years (Hamid, 2005). Similar with laryngotracheobronchitis, it also has its distinct symptom. Patients suffering from this condition often display a sudden distinctive position with the mouth open and the chin thrusting forward. In addition, the patient has a disability while swallowing and displays an extreme anxiety (Porth, 2009).
Lastly, bronchiolitis is another respiratory condition suffered mostly by children below two years. Its symptoms are similar to laryngotracheobronchitis. Its distinctive symptoms faced by the patient include wheezy cough and as well irritability during coughing. In addition, the victim suffers from a mild respiratory distress. Its typical symptoms include breathlessness, shallow breathing and as well retractions (Rush, 2007).
The highlighted respiratory diseases lead to acute respiratory distress. Acute respiratory distress has its typical signs (Smith, 2008). Some of the signs include grunting noises, decreased chest movement and as well chest retractions. On the other hand, patients suffering from respiratory distress display symptoms of fatigue and as well, extreme agitation resulting from interrupted heart activity due to the change in breathing rhythm (Porth, 2009).
References
Rush, B. (2007). Equine Respiratory Diseases. Oxford: John Wiley & Sons.
Hamid, Q., Shannon, J., & Martin, J. (2005). Physiologic basis of respiratory disease. Hamilton: B. C. Decker.
Smith, T. L. (2008). Asthma. New York: Chelsea House Publishers.
Porth, C.M., & Matfin, G. (2009) Pathophysiology: Concepts of altered health states. (Eight ed.) Philadelphia, PA: Lippincott Williams & Wilkins.
Question #1
 While using a metered dose inhaler, there are some descriptions made on the patient. There is a requirement on the patient to use one or two inhalations every four hours. In addition, the patient should not use the inhaler for more than twelve puffs a day (Porth, 2009). The patient should start by shaking the inhaler for five to six times (Gedatus, 2000). Removal of the mouthpiece cover follows. The patient should place the lips and the teeth over the space of the inhaler and breathe in slowly.
While using a metered dose inhaler, there are some descriptions made on the patient. There is a requirement on the patient to use one or two inhalations every four hours. In addition, the patient should not use the inhaler for more than twelve puffs a day (Porth, 2009). The patient should start by shaking the inhaler for five to six times (Gedatus, 2000). Removal of the mouthpiece cover follows. The patient should place the lips and the teeth over the space of the inhaler and breathe in slowly.
In the same time, the patient should squeeze the canister once and keep inhaling after the squeeze. The patient should continue inhaling slowly and deeply, and after inhaling, he should remove the spacer from the mouth where he holds the breath for almost ten seconds. After using the inhaler, there is a prescription of the use of a nebulizer. Nebulizer is a mist that increases the ability of the asthma medication drug inhaled easily into the lungs. This medication applies on patients suffering from severe asthma (Porth, 2009).
Asthma discharge includes a review of the practices used on a patient suffering from asthma. There is need for preventative treatment on a patient suffering from asthma. This starts when asthma symptoms appear on a patient. The child’s family should be able to use the inhaler. With a complete asthma discharge, the family should have an understanding of the management of asthma condition on the child (Porth, 2009).
Acquiring education on asthma management should be through continuous visits to an outpatient clinic. During the time of discharge, there should be prescription on the child. The child gets some scripts displaying the drugs to use where he can easily purchase them from a pharmacy. Establishment of a clear follow up is the other discharge plan. Appointment of the child with a pediatrician give the family a medical review and the progress of the child. Lastly, the family should have an action plan regarding the performance of the child (Porth, 2009). There should be communication between the pediatricians and the family on the action plan developed on the child suffering from asthma.
Question #2
Restrictive airways disease is a condition that affects mostly kids up to the age of five years. The symptoms and signs of this condition are same to those of asthma. Therefore, it becomes hard sometimes to differ between the two (Elling, 2009). The most common symptom is troubling when breathing and this leads to the production of a wheezing sound. The patient may also experience a persistent cough, which does not end easily. A fast heartbeat rate and a running nose are also common in children who have the restrictive airways disease. The infection affects the child’s ability to fight off a common cough and other common illnesses. The infection also leads to the child having a narrow airway because of the swelling of the airway (Gedatus, 2000).
Obstructive lung disease on the other hand is a condition that leads to the shortness of breath which is a result of the difficulty breathing out. The amount of air released from the lungs is much smaller than the normal and therefore, the larger amount of air remains in the lungs. The main symptoms of this disease are fatigue, cough, shortness of breath with less activity, and wheezing (Elling, 2009).
The most common causes of restrictive airway diseases include asthma in the family, and if the child was breastfed for less than three months. If there was no treatment of bronchiolitis at a tender age or any other lung infection then the risk is high. Allergies such as pollen or pets may also trigger the illness (Porth, 2009). There are certain tests used to determine whether a child is suffering from restrictive airway disease (Elling, 2009). The first is the pulse ox meter, measures the amount of oxygen in the blood. Spirometer, used on older children, measures how good a child can breathe. While determining the child’s ability to breathe, there is the use of mucus samples and blood tests.
Question #3
Auscultation refers to the process of identifying the presence of normal breath sounds and as well abnormal sounds. Attaining this is by using a stethoscope (Aehlert, 2011). In addition, there can be a close observation of the patient’s signs of hyperventilation (such as dizziness). Pleural effusion refers to a condition where a patient suffers from abnormal amounts of fluid around the lung. Auscultation on a patient suffering from the condition located on the right lower lobe displays a creaking sound on the right side of the lungs (Gedatus, 2000). These sounds are continuous depending on the level of the fluid in the lungs. In addition, the sounds appear both while the patient is inhaling and as well while exhaling air from the lungs (Aehlert, 2011).
References
Aehlert, B., & Vroman, R. (2011). Paramedic practice today: Above and beyond. St. Louis, Mo: Mosby Jems Elsevier.
Elling, B., Elling, K. M., & American Academy of Orthopaedic Surgeons. (2009).Paramedic: Pharmacology applications. Sudbury, Mass: Jones and Bartlett Publishers.
Gedatus, G. M., & Dolan, C. (2000). Mononucleosis. Mankato, Minn: LifeMatters.
Porth, C., Matfin, G., Barkman, A., & Pooler, C. (2009). 26: Heart failure and circulatory shock. Pathophysiology: Concepts of Altered Health States
Patient discharge plans for asthmatic patient plans are quite challenging due to the complexity of the health situation. The use of nebulizers and metered dose inhaler require competency. Inhaler therapy entails educating the patient on the best inhaler practices.
To establish a discharge plan for the 6-year-old child with asthma, it is vital for the nurse practitioner to educate the patient on the use of the metered dose inhalers. First, the metered dose inhaler has a softer taste from other inhalers, thus patients who have used other inhalers before may over use the inhaler on thought that the inhaler is not reaching the lings. Consequently, metered dose inhalers require proper cleaning and priming before using them for the first time.
While using the inhaler, the patients should shake the inhaler for relatively five seconds. The inhaler is primed by pressing the canister down to release medication. However, patients should avoid holding the inhaler close to their faces to prevent the medication from reaching the eyes.
Asthma therapy for nebulizers requires protocol. Nebulizers require careful patient education on how to assemble the nebulizer cup and the mouthpiece. In addition, patients should assume an appropriate posture while using nebulizers. Their backs should be straight and if the child is young or requires help, they should sit on the adults lap in an appropriate posture (Porth, Matfin, Barkman, & Pooler, 2009).
Consequently, since the patient is of young age, the nurse practitioner should also educate his parents or guardians on the proper asthmatic practices. The child may require extra help during an asthmatic attack, thus parental health education on the child’s health practices is important.
Obstructive and restrictive lung diseases have many symptoms in common. For instance, they entail breath shortness with exertion. Victims with restrictive lung diseases find it difficult filling their lungs with air. Their lungs muscles cannot expand fully. On the other hand, people with obstructive lung disease have trouble in exhaling air from their lungs. This is mostly caused by narrowed airways.
Patients with restrictive lung disease experience lung stiffness, weak lung muscles or damaged nerves. These conditions restrict lung expansion thus leading to breathing complications. Obesity, scoliosis, interstitial lung diseases and neuromuscular diseases are the main causes of lung diseases (Aehlert & Vroman, 2011).
The diagnosis of restrictive lung diseases starts with a pulmonary function tests. Consequently, the diagnosis includes laboratory testing and physical examination. Image tests including chest X-rays and computed chest tomography are also vital in restrictive lung disease diagnosis.
Normal lung sounds are heard from bronchial breathing and vesicular breathing. Nurses listen to different breath sounds from the bottom to the top of the chest. The stethoscope tests assess the symmetry, intensity, length of expiration and inspiration. Consequently, medical practitioners compare breath sounds between the lower and the upper chest in an upright position.
In an abnormal breathing test, lack of intensity symmetry on one side of the chest may be detected. Pleural effusion may lead to abnormal chest sounds. If the pleural effusion is located at the right lower lobe, breathing sounds become diminished or even absent. Pleural effusions compress the large central airways in the lungs. Further, the effusions loosen the lungs elastic tension. These factors lead to diminished breathing sounds (Light, 2007).
References
Light, R. W. (2007). Pleural diseases. Philadelphia: Lippincott Williams & Wilkins.
Aehlert, B., & Vroman, R. (2011). Paramedic practice today: Above and beyond. St. Louis, Mo: Mosby Jems Elsevier.
Porth, C., Matfin, G., Barkman, A., & Pooler, C. (2009). Heart Failure and Circulatory Shock. New York, N.Y: Penguin Books.
Browse More Essay Topics 24/7/365 Support 11+ Yrs in Essay Writing Pay for Quality not Quantity Score that A+ Grade