+1(209) 348-9544
order@myessayservices.com
+1(209) 348-9544
order@myessayservices.com
![]() Every academic student understands clearly how challenging it can be to meet a tight deadline. Once you are short of time, and the task should be done within some time lag, you may end up asking yourself: “Is there anyone who can help write my research paper at a small fee?” That’s where My Essay Services.com can be your perfect choice. Whether your a PhD, Masters, College High School or Bachelors we can deliver an original paper as per your instructions.
Every academic student understands clearly how challenging it can be to meet a tight deadline. Once you are short of time, and the task should be done within some time lag, you may end up asking yourself: “Is there anyone who can help write my research paper at a small fee?” That’s where My Essay Services.com can be your perfect choice. Whether your a PhD, Masters, College High School or Bachelors we can deliver an original paper as per your instructions.
When you buy an essay online from us, we offer you an original, nil plagiarized and unique paper written by a dedicated writer who is PhD or Masters qualified. My Essay Services is an experienced service with over 9 years experience having delivered over 83,000 essays over the years.


History of Present Illness
 S.E is a business manager who explains that he has been experiencing shoulder pains and stiffness. He explains that the problem started six months ago. However, the his condition was previously mistaken for musculoskeletal and he was referred for physical therapist treatment. The patient now presents with a stiffness in the right shoulder extending into the elbow and a resting tremor in the right and left hand. He was referred to a neurologist and he was diagnosed with early Parkinson’s Disease.
S.E is a business manager who explains that he has been experiencing shoulder pains and stiffness. He explains that the problem started six months ago. However, the his condition was previously mistaken for musculoskeletal and he was referred for physical therapist treatment. The patient now presents with a stiffness in the right shoulder extending into the elbow and a resting tremor in the right and left hand. He was referred to a neurologist and he was diagnosed with early Parkinson’s Disease.
Current Medications
Ropinirole 5mg p.o TID.
Parkinson’s Disease
Parkinson’s disease occurs because of loss of dopamine; a chemical produced by the brain that helps in facilitating movement. Furthermore, dopamine also affects one’s mood. Thus, medications for the Parkinson’s disease entail prescription of pills that replace dopamine in the body.
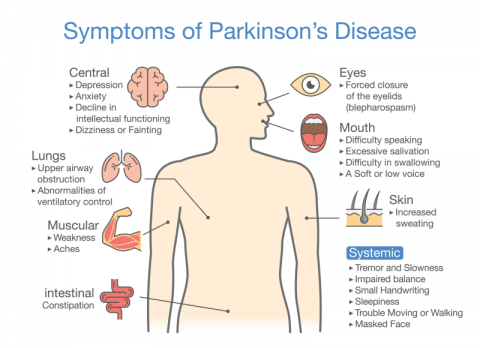
Parkinson’s disease presents with various signs and symptoms. However, symptoms are different among patients. Some patients show early stages symptoms, while others start showing symptoms during the later stages. Normally, symptoms for the disease present in individuals who are aged between 50-60 years. Symptoms develop gradually and the close family may not notice anything wrong with the patient. Parkinson’s disease can cause motor or non-motor symptoms. Motor symptoms involves symptoms that affect movement, whereas non-motor symptoms do not affect movement (Kalat, 2013).
Motor symptoms
Motor symptoms for Parkinson’s disease include tremors. Tremors are the most frequent symptoms of the disease. Tremors in Parkinson’s disease may affect only one leg or arm. Moreover, other patients present with tremors experienced on one side of their body. The tremors can also be felt in the lips, chins and tongues. When the disease progresses, the tremors can be felt on both sides of the body. However, in other patient’s the tremor remains in one side of the body even in the later stages of the disease. Other motor symptoms include aching muscles and stuff muscles, slowed or limited movement, problems with walking and balancing and weakness felt in the face and throat muscles. Furthermore, other patients may experience freezing or a sudden inability to walk (Lavretsky, Sajatovic & Reynolds, 2013).
Non-motor symptoms
Non-motor symptoms for the disease include constipation, depression and sleep problems
Patients who have received a patient diagnosis previously may experience end-of-dose effects, which affect the motor performance. This occurs because the effects of motor improvement by levodopa dosage fluctuate with time and the Parkinsonism reappears. Moreover, these end-of-dose effects may also manifest in other symptoms like anxiety, excessive sweating, akathisia and depression. Moreover, dyskinesias can also hinder the management of the Parkinson’s disease. Dyskinesias is an involuntary movement that occurs in response to dopamine or levodopa agonist intake. Dyskinesias mostly occurs at peak-dosage levels (Lavretsky, Sajatovic & Reynolds, 2013).
The diagnosis or therapeutic management of motor complications depends on the movement complications experienced. Treatment of the Parkinson’s disease can be performed with two approaches. The first approach aims at improving the dopamine levels in the brain. On the other hand, the second approach aims at improving the symptoms caused by the Parkinson’s disease. Patients with the disease can receive medication to eliminate the symptoms experienced. Moreover, if the remedy is redundant after medication, patients can also chose to undergo a safe surgical treatment. The treatment for Parkinson’s Disease is done by neurologists who are movement disorders specialists.
The drugs used to diagnose Parkinson’s disease include levodopa. Levodopa is commonly prescribed to control the symptoms caused by the disease mostly, rigidity and bradykinesia. Once levodopa gets into the body, it is transported to the nerve cells present in the brain that produce dopamine. Levodopa is then converted into dopamine. The side effects for using levodopa include disturbances of the heart rhythm, nausea and vomiting. Consequently, if levodopa is used in the long-term, levodopa can cause abnormal movements, restlessness and confusion (Weiner, Shulman & Lang, 2013).
Further, doctors can prescribe dopamine agonists to manage Parkinson’s disease. Dopamine agonists include bromocriptine, pramipexole and ropinerole. The dopamine agonists are used to produce a dopamine-effect in the brain. However, these agonists do not produce dopamine, they mimic the effect of dopamine. Dopamine agonists cause less motor fluctuations than levodopa or carbidopa. Further, they do not induce any protein effects. Nevertheless, there are many complications caused by the use of dopamine agonists. For instance, dopamine agonists have not yet been proved to slow the progress of Parkinson’s disease. Moreover, these agonists are not as effective as carbidopa and levodopa in treating motor symptoms. Side effects include hallucinations, sexual obsessions and daytime sleepiness (Kalat, 2013).
Sinemet is another drug prescribed to treat Parkinson’s disease. Sinemet is comprised of levodopa and carbidopa. Levodopa gets into the brains cells and is converted into dopamine. On the other hand, carbidopa increases the effectiveness of levodopa. In addition, it reduces the side effects caused by levodopa. Doctors can engage patients in either sinemet immediate-release or controlled-release. Both of these medications are effective in managing the Parkinson’s condition. Although most people prefer the controlled release sinement medication, doctors can advise you on which one is best for you (Lavretsky, Sajatovic & Reynolds, 2013).
Sinemet CR 200mg/50mg The dosage may be split and taken at half the dosage listed. To reduce the motor effects on the patient.
Prolopa 50mg/200mg Should be taken in existing form. Used to add levodopa in the patient.
Tasmar 100mg or equivalents Tasmar should be taken in existing form. Prolongs the effectiveness of levodopa
References
Lavretsky, H., Sajatovic, M., & Reynolds, C. F. (2013). Late-life mood disorders. Oxford: Oxford University Press.
Weiner, W. J., Shulman, L. M., & Lang, A. E. (2013). Parkinson's disease: A complete guide for patients and families.
Kalat, J. W. (2013). Biological psychology. Belmont, CA [etc.: W
 Parkinson’s disease is one of the diseases that affects millions of people in the United States alone. I was therefore, interested in the way this disease worked and the way it affects persons. I was especially interested in its relation with the endocrine system as there were several studies that had showed there was a relation between the two. Therefore, this made this topic more interesting and I wanted to find more information regarding it. It is through this literature that I stumbled upon an article on endocrinology. I found an article that discussed the effect of Parkinson disease on the endocrine system and dysfunction of the system. The whole idea was important to me as I wanted to understand the information better and understand the correlation that existed between the two. The article was on a study regarding the prevalence of endocrine dysfunction in subjects with idiopathic Parkinson’s disease referred to as IPD on the newer dopaminergic agents (DA). The article discussed whether indeed the Parkinson’s disease was related to newer dopaminergic agents.
Parkinson’s disease is one of the diseases that affects millions of people in the United States alone. I was therefore, interested in the way this disease worked and the way it affects persons. I was especially interested in its relation with the endocrine system as there were several studies that had showed there was a relation between the two. Therefore, this made this topic more interesting and I wanted to find more information regarding it. It is through this literature that I stumbled upon an article on endocrinology. I found an article that discussed the effect of Parkinson disease on the endocrine system and dysfunction of the system. The whole idea was important to me as I wanted to understand the information better and understand the correlation that existed between the two. The article was on a study regarding the prevalence of endocrine dysfunction in subjects with idiopathic Parkinson’s disease referred to as IPD on the newer dopaminergic agents (DA). The article discussed whether indeed the Parkinson’s disease was related to newer dopaminergic agents.
The article studies the prevalence of endocrine dysfunction in subjects that had the Idiopathic Parkinson disease (IPD) on newer dopaminergic agents. The Idiopathic Parkinson’s disease (IPD) is often characterized by the dopamine deficiency in the basal ganglia. It is important to note that Levodopa (a dopamine precursor) and dopaminergic agents can be described as being useful in IPD treatment (Endocrine Society, 1917). It is of crucial importance to note that the hypothalamic neurotransmitter plays an important role in the regulation of hormones some of which might be of relevance in IPD. The neurotransmitter deficiency in this region is consequently of considerable interest. The link between potential hormonal perturbations and non-motor symptoms of IPD is of interest but currently it remains extremely speculative. Therefore, article looked at the prevalence of endocrine dysfunction in subjects with idiopathic Parkinson disease.
There are only limited number of prospective studies of long-term DA use and the endocrine function. Therefore, the research wanted to understand the relation between the DA use and the endocrine function. In fact, with the introduction of new dopaminergic such as rotigotine, ropinirole and pramipexole there has been little research into this phenomena and this is the premise by which the research was carried out. The studies that have been done have led to conflicting results and therefore, the researchers felt that it was important to study the endocrine function in subjects that had IPD medication-induced hormonal perturbations which when left might led to worsening of non-motor effects of IPD and consequently contribute to a poor quality of life.
The paper is about the prevalence of endocrine dysfunction in subjects that have idiopathic Parkinson’s disease. Therefore, the article is about the endocrine system and consequently endocrinology. It discusses the endocrine system is affected by the disease and how it cannot normally function. It is of the essence to understand that indeed the Idiopathic Parkinson’s disease affects the endocrine system as it affects the basal ganglia. It affects dopaminergic agents which are a part of the endocrine system. They also cause hormonal perturbations and non-motor symptoms. Dopamine receptors are often expressed in the endocrine tumor cells and normal endocrine cells (Endocrine Society, 1917). Therefore, the Dopamine receptors have a potential to inhibit hormone secretion and consequently affect the whole endocrine system.
The research team recruited 25 subjects that had IPD attending the Parkinson’s disease clinic and they have informed consent. The subjects were aged over 40 years and had been on DA for more than six weeks. The method that was used in the research was a cross-sectional study, where the research team measured the insulin like growth factor-1, follicle stimulating hormone, luteinizing hormone, thyroid function, cortisol and testosterone and cortisol levels. The tests were done by simply following a short synacthen rest. All the subjects were studied for thirty minutes after inserting an intravenous cannula and blood was collected for insulin growth factor, follicle stimulating hormone and thyroid stimulating hormone. Therefore, from this methodology the researchers were able to understand whether or not patients that had IPD had endocrine dysfunctions. The methodology worked in a way that the persons were diagnosed for IPD to ensure that indeed they had it and all the endocrine hormonal secretions were looked at. They were measured and it was determined whether there existed abnormalities in their levels. There was the use of a control group that ensured that the experiment was able to remain on track and that there variations that were seen were not caused by any other problem other than the endocrine situation.
The research generated key results by looking at the patients and measuring their levels of hormones. All the subjects were studied between 9 and 9.30 A.M each and every day and the samples were taken then centrifuged and the plasma stored until it was assayed. The statistical analysis for the results were done and the statistical advice on numbers were obtained from a statistical advisor of the Aneurin Bevan University Health Board. Further, the summary data that were seen to be non-normally distributed and were compared using non-parametric methods and the data tables were compared with a chi-square test using IBM SPSS. In the study, there were about 18 males and around 7 females in the study that had a median age of around 72 years. The median time to study that was used from the IPD diagnosis was 27 months and interquartile range 17-45. There were a variety of DA that included ropinirole, rotigone, as well as pramipexole. The Endocrine function was entirely normal using the study protocol in the 19 subjects that were looked at in the recruitment.
However, it is important to understand that in the study two to three subjects had persistent abnormalities. There were no significant differences in the demographic details, the treatment in those that had suppressed PRL and the duration of IPD. These key results were used in the research and they were used to ensure that indeed the research questions was answered. The results were sufficient to ensure that the hypothesis was able to be answered in a correct manner (Endocrine Society, 1917). In the study, the results showed that the newer DA do not in any way cause significant endocrine dysfunction in subjects that had IPD even when they were given a median period of around 27 months. In fact, 92% of the subjects had an entirely normal endocrine function at recruitment or at repeat testing together with normal pituitary structure when the complete imaging was done. Further, 96% of the subjects had a normal cortisol response to ACTH during the SST. However, it is important to note that there was a significant suppression of PRL in around 44% of these individuals, however, they were within the reference range.
The results were able to justify the conclusion, in that they showed that the newer DA do not often cause significant endocrine dysfunction.
The Cortisol response was normal in 24 out of the 25 patients at recruitment. However, they could not be able to be further investigated in the only subject that had a minor abnormality. On the other hand, eleven of the 25 subjects that is 44% had what can be said to be isolated suppressed PRL levels and the reference rage was about 40-530 IU/L. It is imperative to understand that a comparison of subjects with suppressed PRL with those with normal PRL was not able to show any significant differences in weight gender and age. There was also a significant difference in time from the diagnosis of IPD in different durations of treatment for IP between the two groups. However, there was a significantly higher number of subjects that had suppressed PRL levels were on DA therapy and they were compared to the number of subjects with PRL in the reference rage. Therefore, the endocrine function can be said to be entirely normal with all the persons. The results were therefore, able to justify the conclusion that there were newer non-ergoline DA therapy that was caused only minimal endocrine perturbations in the subjects that had IPD (DeGroot,1989). Therefore, the clinical significance can be described as only being speculative, further, the results showed that the cortisol response to ACTH was normal in all the persons but a significant minority that had suppressed prolactin levels.
The first question that I asked myself about the Idiopathic Parkinson’s disease is why there was a need to correlate Idiopathic Parkinson’s disease with the endocrine system. As I read the article I wondered why long DA use affected the endocrine function in IPD and why IPD alone. I did not understand whether there some clinical cases that existed in the hospital where the persons that had IPD were diagnosed with endocrine dysfunctions because of extensive DA use. I tried to research on the subject but there was no information in regards to this subject and consequently, the questions still lingered. I kept asking myself was why it was necessary to study the relationship between DA use and the endocrine function in IPD. The second question was why some three subjects had persistent abnormalities. They had elevated PRL level but a normal pituitary CT scan, secondly they had undetectable IGF-1 levels with normal endocrine tests, but the subjects at some time defaulted several times from pituitary imaging. A third question was that disturbed me was whether the tests might have led to the death of the third subject. This is because there was a need to ensure that indeed the normal endocrine profiles were put into good use and the monitoring might have triggered something.
The fourth question was why there was a significant suppression of PRL in 44% of the individuals; with the reference range of about 56%. Why did this happen, I believe that there is a need for further research in order to ensure that indeed ones understand this correlation and why it exists. There is research that argues that the expected effect of high dose DA therapy might have caused the significant suppression of PRL. However, being an isolated phenomenon and there were no accompanying endocrine abnormalities. The fifth question is whether there was a correlation between SST and other pituitary abnormalities as demonstrated with one subject. This is because even previous research and reports on hypothalmo-pituitary axis (HPA) in treatment naïve as well as treated subjects with IPD had shown different and conflicting results (Aquilonius, 1984). Further, one of the limitation of the study was that there was no large number of subject that could have given the research statistical credibility regarding the results. Therefore, that one subject might have represented thousands of persons that showed those similar symptoms but because of the limited statistical credibility and number of subjects it was extremely difficult to prove.
It is important to understand that there several limitations to the study, firstly, a larger number of subjects would have given more statistical credibility to the results. The figure of 25 was extremely low and consequently, it was difficult to determine whether one subject had a problem or it was the whole population (M, J. S., 2000). The other limitation was the fact that there was the lack of dynamic pituitary test in order to detect subtle pituitary dysfunction. The last limitation is that the research had the inability to relate low prolactin levels to non-motor manifestations of IPD and this was because of the study design. However, the research argued that there was a need to ensure that the main message was not retracted because of these limitations.
Reference
Endocrine Society., & Association for the Study of Internal Secretions (U.S.). (1917). Endocrinology. Los Angeles, Calif: Association for the Study of Internal Secretions.
DeGroot, L. J. (1989). Endocrinology. Philadelphia: Saunders.
Aquilonius, S.-M. (April 01, 1984). THEORIES OF TRANSMITTER DYSFUNCTION IN DISORDERS OF THE BASAL GANGLIA. Acta Neurologica Scandinavica, 69, 32-40.
M, J. S., M, W.-P., & D, H. G. (December 01, 2000). The Genetics of Frontotemporal Dementia and Related Disorders. Current Genomics, 1, 4, 339-352.
1.0 Introduction and definition of terms
 Ehrlichiosis is a general term used to refer to a collection of arthropod-borne diseases that are particularly spread by ticks (Vector). Arthropods refer to invertebrates with external skeleton (exoskeleton), jointed appendages and segmented body. They include arachnids, insects and crustaceans. On the other hand, a vector is an organism (usually an arthropod) that transfers a pathogen from one organism (host) to another. Biological vectors are those that harbor the ineffective agent in their bodies and the agent multiplies and develops in the vector before being actively transferred.
Ehrlichiosis is a general term used to refer to a collection of arthropod-borne diseases that are particularly spread by ticks (Vector). Arthropods refer to invertebrates with external skeleton (exoskeleton), jointed appendages and segmented body. They include arachnids, insects and crustaceans. On the other hand, a vector is an organism (usually an arthropod) that transfers a pathogen from one organism (host) to another. Biological vectors are those that harbor the ineffective agent in their bodies and the agent multiplies and develops in the vector before being actively transferred.
In this case, the vector is essential to the pathogen’s life cycle, classical examples are ticks, mosquitoes, lice and fleas. In contrast, the mechanical vector is not vital for the pathogen’s lifecycle because it merely picks the pathogen on the surface of its body and transfers the pathogen passively. A typical example is a housefly which may pick pathogens on its appendages upon landing on feces and transfer it to food before consumption (Farlex, Inc.). Ehrlichiosis is mainly transmitted by four tick species Dermacentor variabilis, Amyblyomma americanum (lone star tick), Ixodes scapularis and I. pacificus which are widely distributed in the United States, Latin America, New England and Africa (Keesing, Hersh, & Ostfeld, 2012)
2.0 Etiology and Microbiology of the pathogen
The etiology of Ehrlichiosis in humans has been linked to five bacteria species of the Anaplasmataceae family i.e. Ehrlichia/Anaplasma phagocutophilium (causes human granulocytic ehrlichiosis/anaplasmosis), E. chaffeensis (associated with human monocytic ehrlichiosis), E. ewingii (responsible for human ewingii ehrlichiosis), E. canis and E.sennetsu (linked to sennetsu fever) (Dumler, et al, 2005a; Goddard, 2008). However, only the first three have been elaborately studied.
Recently, another species (provisionally refered to as E. muris-like wasisolated from a few patients travelling from Wisconsin and Minnesota but the vector for this species has not been identified (CDC, 2013). The pathogens responsible for ehrlichiosis target circulating leucocytes and thus the corresponding diseases are named as per the leucocytes infected by the specific bacteria. For instance, the human monocytic ehrlichiosis (HME) is caused by E. chaffeensis which infects monocytes while human granulocytic anaplasmosis (HGA), formerly HGE (ehrlichiosis) is caused by A.Phagocytophilum which attacks granulocytes. E. ewingii infects neutrophils and is serologically similar to E. chaffeensis (Dumler, et al, 2005a).
The bacteria responsible for ehrlichiosis are gram-negative coccobacilli (ellipsoidal in shape) (Ismail, Bloch, & McBride, 2010; Lyme and Tick-Borne Diseases Research Center , 2011). That means that in the decolorization with alcohol they lose the primary crystal violet-iodine stain but retain the safranin counter stain and they have a thinner cell wall (with only 10% peptidoglycan). In addition, gram-negative bacteria have an outer lipid membrane separated from the cell wall by a periplasmic space (Aneja, Jain, & Aneja, 2009).
In addition, the bacteria are obligate intracellular parasites, meaning that they rely on the cellular resources of the host for their growth and reproduction and thus can only grow and reproduce in the host (Aneja, Jain, & Aneja, 2009). The bacteria occupy cellular cytoplasmic vacuoles in the host in microcolonies referred to as morulae which can be observed under a microscope as below (figure 1 and 2)
3.0 Reservoir, Transmission, epidemiology
The Ehrlichia genus is found in many vertebrate reservoirs, in which it multiplies without causing disease. The most common vectors include the white tailed deer, goats, domestic dogs, red foxes and several bird species (Ganguly & Mukhopadhayay, 2008). A study aimed at establishing the vector competence of A. phagocytophilum assessed 4,640 ticks that were collected over a period of 3 years from 254 animals. The study found that small mammals were the most competent reservoirs and identified more reservoirs including eastern chipmunks, white-footed mice, short-tailed shrews, opossums, skunks and southern flying squirrels (Keesing, Hersh, & Ostfeld, 2012).
Ehrlichiosis is transmitted through tick bites. The larvae stage of the ticks pick the causative bacteria from a vertebrate reservoir during a blood meal and maintain it through the nymphal stage which may transmit the bacteria to another reservoir or to humans during a blood meal. In addition, an adult tick may acquire the bacteria from infected nymphal stage through trans-stadial transmission or during a blood meal and pass it to another host (Ganguly & Mukhopadhayay, 2008). Below is the transmission cycle of the disease.
As earlier implied there are three main diseases that form the collection of ehrlichiosis and of the three earlier mentioned, human monocytic ehrlichiosis (HME) and human granulocytic anaplasmosis (HGA) are the most common in the United States. The former was first described in humans in 1987 while the latter was described in 1990s (Dumler & Walker, 2009; Vorvick, 2011). However, A.phagocytophili, causative agent for HGA, had been identified as a veterinary pathogens as early as 1932 and was common in horses, dogs, sheep, cats and goats (Dumler, et al., 2005b).
Currently, HME is found in 30 states mainly in the mid-Atlantic, southeast and south-central states as well as in parts of Africa and Europe. On the other hand, HGA is found in the mid-Atlantic, northeast, Midwest states, many parts of Europe and northern California. Unfortunately, because of inaccurate reporting and difficulties in diagnosis, the actual prevalence of the disease is unknown but is estimated to be between 15% and 36% in the endemic areas goats (Dumler, et al., 2005b). Some researchers have found that E.chaffeensis is endemic in the south central and south eastern states and of great public health significant thus a reportable disease with about 0.7 HME cases per million population being reported every year.
If untreated or treated late, HME is fatal with a mortality rate of about 2.7%. Of the reported cases of HME. 75% are men at an average age of 44 years and mostly living in the rural areas. On the other hand, HGA is endemic in north central and pacific states and New England. 1.6 cases of HGA per million population are reported every year. E. ewingii (responsible for human ewingii ehrlichiosis) is more common in dogs and only found in a few immunocompromised individuals. E. ewingii is endemic in south Atlantic and south central states and causes mild illness that is similar to HME and has not been linked to any fatality (Goddard, 2008).
4.0 Pathophysiology, pathogenesis, symptoms, diagnosis and treatment
Unlike most of the other common human bacteria pathogens, Ehrlichia lack pili and thus they bind to the specific host cells, mentioned earlier, through their membrane and enter (infect) the cells (Paddock & Childs, 2003). Once in the cell the bacteria form 1or 2 endosomes (membrane bound compartments) referred to as morulae, but they can be as many as 15 in an immunocompromised patient (Ganguly & Mukhopadhayay, 2008; Ismail, Bloch, & McBride, 2010). Though Ehrlichia mainly infect monocytes, they have been reported to infect lymphocytes, metamyelocytes, neutrophils and promyelocytes (Nicholson, et al., 2010).
They multiply within the endosome and survive by suppressing the host immune system hence they are often linked to immunosuppression which in turn may lead to multi-organ infection and failure. Infections in the lymph nodes, bone marrow, liver, pariearteriolar sheaths and splenic chords have been reported in humans (Paddock & Childs, 2003). The multiple systems and organ infection, particularly in the bone marrow, is common in late stages of the disease and in immunocompromised individuals). (Paddock & Childs, 2003; Ganguly & Mukhopadhayay, 2008; Shipo, Klement, Tagar, Waner, & Harrus, 2008; Ismail, Bloch, & McBride, 2010; Nicholson, et al., 2010).
My cousin was diagnosed with HME and displayed the following symptoms rushes, muscle aches, fatigue, headaches, chills, confusion, red eyes, nausea, diarrhea and vomiting associated with include. The same symptoms are associated with HGA and others include myalgia, malaise, respiratory, GI and CNS abnormalities. The disease is also associated with immuno-suppression and thus opportunistic infections such as candidiasis are common (Goddard, 2008).
Several diagnostic tests for ehrlichiosis are available and include micrsoscopy, PCR amplification, serological tests such as western blotting and indirect immunofluorescence assay (IFA) (Ganguly & Mukhopadhayay, 2008). Blood cultures may also be used for diagnosis. Once the disease has been identified as ehrlichiosis it is treated with doxycycline or rifampin. Other treatments include chloramphenical and tetratcyclines. Tick control, avoiding long grass and bushes, tick removal, using insect repellants and protective cloths when handling animals are the main preventive strategies (CDC, 2013).
References
American Lyme Disease Foundation. (2010, January 5). Other Tick-Borne Diseases: Ehrlichiosis.
Aneja, K., Jain, P., & Aneja, R. (2009). A Textbook of Basic and Applied Microbiology . New Delhi: New Age International Pvt Ltd Publishers .
CDC. (2013, September 5). Ehrlichiosis: Symptoms, Diagnosis, and Treatment.
Dumler, J. S., Madigan, J. E., Pusterla, N., & Bakken, J. S. (2005). Ehrlichioses in Humans: Epidemiology, Clinical Presentation, Diagnosis, and Treatment. Clinical Infectious Diseases , 45 (1), 45-51.
Dumler, J., & Walker, D. (2009). Ehrlichia chaffeensis (human monocytotropic ehrlichiosis), anaplasma phagocytophilum (human granulocytotropic anaplasmosis), and other anaplasmataceae. In G. Mandell, J. Bennett, & R. Dolin, Principles and Practice of Infectious Diseases (p. chap 193). Philadelphia, Pa: Churchill Livingstone Elsevier.
Dumler, J., Choi, K., Garcia-Garcia, J., Barat, N., Scorpio, D., Garyu, J., et al. (2005). Human granulocytic anaplasmosis and Anaplasma phagocytophilum. EMERGING INFECTIOUS DISEASES , 11 (12), 1828-1834.
Farlex, Inc. (n.d.). vector.
Ganguly, S., & Mukhopadhayay, S. K. (2008). Tick-borne Ehrlichiosis infection in human beings. Vector Borne Diseases , 45, 273-280.
Goddard, J. (2008, September 1). What Is New With Ehrlichiosis?
Ismail, N., Bloch, K. C., & McBride, J. W. (2010). Human Ehrlichiosis and Anaplasmosis. Clinics in Laboratory Medicine , 30 (1), 261-92.
Keesing, F., Hersh, M. H., & Ostfeld, R. S. (2012). Reservoir Competence of Vertebrate Hosts for Anaplasma phagocytophilum. Emeging Infectious Diseases , 18 (12), 2013-2016.
Lyme and Tick-Borne Diseases Research Center . (2011). EHRLICHIOSIS/ANAPLASMOSIS.
Nicholson, W., Allen, K., E McQuistonWilliam L. Nicholson1, E.-m. t., Allen, K. E., McQuiston, J. H., Breitschwerdt, E. B., et al. (2010). The increasing recognition of rickettsial pathogens in dogs and people. Trends in Parasitology , 26 (4), s 205–212.
Paddock, C., & Childs, E. (2003). Ehrlichia chaffeensis: a Prototypical Emerging Pathogen. Clinical Microbiology Reviews , 16 (1), 37–64.
Shipo, V., Klement, A., Tagar, E. R., Waner, T., & Harrus, S. (2008). Prognostic indicators for canine monocytic ehrlichiosis. Veterinary parasitology , 153 (1-2), 131-138.
Vorvick, L. J. (2011, August 24). Ehrlichiosis.
Browse More Essay Topics 24/7/365 Support 11+ Yrs in Essay Writing Pay for Quality not Quantity Score that A+ Grade