+1(209) 348-9544
order@myessayservices.com
+1(209) 348-9544
order@myessayservices.com
![]() Are you in High School, College, Masters, Bachelors or Ph.D and need someone to help write your paper? All you need is to ask for research paper help written by a specialist in your academic field. When you buy an essay online from us, we offer you an original, nil plagiarized and unique paper written by a dedicated writer who is PhD or Masters qualified. MyEssayServices.com is an experienced service with over 9 years experience having delivered over 83,000 essays over the years.
Are you in High School, College, Masters, Bachelors or Ph.D and need someone to help write your paper? All you need is to ask for research paper help written by a specialist in your academic field. When you buy an essay online from us, we offer you an original, nil plagiarized and unique paper written by a dedicated writer who is PhD or Masters qualified. MyEssayServices.com is an experienced service with over 9 years experience having delivered over 83,000 essays over the years.

Importance of bone density tests
 Osteoporosis is more prevalent on old women relatively at the age of 50. If a patient has osteoporosis or signs of osteoporosis, then bone density tests will determine whether the disease is already established or it is still developing. Bone density tests enable the patient discover a developing osteoporosis condition before ones breaks a bone. Further, bone density tests can help one avoid developing osteoporosis or examine whether your bone density is improving or deteriorating.
Osteoporosis is more prevalent on old women relatively at the age of 50. If a patient has osteoporosis or signs of osteoporosis, then bone density tests will determine whether the disease is already established or it is still developing. Bone density tests enable the patient discover a developing osteoporosis condition before ones breaks a bone. Further, bone density tests can help one avoid developing osteoporosis or examine whether your bone density is improving or deteriorating.
Types of bone density tests
Bone density tests are carried out using a tool called FRAX. FRAX enables physicians calculate the level of osteoporosis prevalence on a person. The results of a bone density test are produced using T-scores. T-scores scale the level of bone density, whether its high or low, by comparing one’s bone density with that of a healthy adult at the age of 30 (Hamdy & Lewiecki, 2013).
Clinical situation
In my clinical situation, where a woman at the age of 60 has been diagnosed with osteoporosis, various medication procedures are necessary. Multiple practices help one reduce their level of osteoporosis development and improve their T-scores. First, the physician can give the patient bisphosphonates. Bisphosphonates reduce the level of bone breakdown or removal. This medication is used to treat osteoporosis in postmenopausal women by treating or preventing osteoporosis.
Further, if the osteoporosis condition is not yet fully developed, the physician can engage the patient in estrogen therapy. Bone density widely reduces among women who are post menopause. Estrogen treatment controls effects of menopause. In addition, synthetic calcium can be given to the patient to improve the calcium concentration in the patient’s body (Hamdy & Lewiecki, 2013).
Consequently, it is important to educate the patient on the risk factors causing the disease condition in order to contain the osteoporosis condition. The risk factors that may lead to development of osteoporosis include, low calcium intake, low vitamin D intake, lack of regular exercises, lifestyle factors and protein intake. Lifestyle factors involve unhealthy behaviors such as cigarette smoking and alcohol consumption (Porth & Mattfin, 2009).
Question 2
Sprains and strains are soft tissue diseases that result from soft tissue injury. The treatment for sprains and strains mainly entails three medical procedures; price therapy, avoiding harm and drug prescription.
Clinical situation
In my medical situation where a 15-year-old child has a knee injury that presented itself 3-4 days ago various medical practice are necessary. First, the patient has a swelling on the inferior portion of the patella. This clearly indicates that the injury is a sprain. The sprain has developed for quite some time before treatment. Thus, price therapy is necessary to prevent further progress of the sprain. Price therapy entails practices aimed at protecting, resting, icing, compression and elevation (Sussman & Bates-Jensen, 2007).
Protecting entails protecting the injured part from further injury. Thus, since the sprain has developed for a couple of days, it should be protected from further injury. The patient explains that the sprain injury came when he was playing basketball. Therefore, the child should refrain from playing the game in order to prevent further complication of the injury. This practice is referred to as resting (Porth & Mattfin, 2009).
The swollen part should be applied cold to reduce the swelling. Furthermore, the injured part should be compressed by wrapping the injured part to avoid further welling. Compression is done by using bandage or any medical wrapping material. Price therapy also entails elevation of the injured part. The injured part should rest on an elevated surface, such as a pillow, in order to reduce the swelling of the injury (Porth & Mattfin, 2009).
Consequently, another way to diagnose the sprain is by avoiding harm. This therapy enables the patient to avoid getting more harm by avoiding heat, alcohol, running and massage. These practice helps improve the speed of healing and the complexity of the injury. Drug prescription is necessary to improve the patient’s condition. The patient is of a young age, and the pain from the sprain should be maintained by using painkillers.
Question 3
Young children of the age 1-3 years normally show gait abnormality in their walking patterns. According to physicians, gait-walking condition is normal in children between 1-3 years old. However, if the condition continues when the child reaches the age of 3 years, then the parents should seek medical help.
Clinical situation
In my clinical situation where the patient is 3 years old, and he shows traits of gait abnormality, I would advise the parent to undergo various examination practices to figure out the seriousness of the condition. As a medical practitioner examining the child’s conditions various practices come into play. First, the medical practitioner should examine the patient’s medical history. The medical history covers the pregnancy condition of the mother when she was carrying the child, the conditions within which the child was born and development of the child. The medical history of the child may enable the medical practitioner know how to diagnose the patient. Further, family history may reveal if there is a familial tendency of developing gait (Duque & Kiel, 2008).
In addition, the medical practitioner should examine the child’s condition whether it is really gait or just mere appearance of the child’s walking pattern. The physician should examine the signs and symptoms of gait on the child for certainty. Further, the physician should examine the child’s sitting habits and aggravating factors such as fatigue on the patient. These practices enable the physician develop the right diagnosis for the child.
Diagnosis for pathological disorders
Diagnosis for pathological disorders involves height and weight assessment. Children who have normal size for their age are less likely to develop pathological conditions such as rickets or hypophosphataemic. In addition, the diagnosis should also entail musculoskeletal assessment. Musculoskeletal assessment involves examination of the spine, leg length, the shape of the feet whether they are flat for normal walking or not, examination of the lower extremities and examination of the ankle dorsiflexion with regards to the neutral position in order to examine whether the child has foot deformity (Duque & Kiel, 2008).
Neurological assessment is also vital for examining pathological child disorders. Neurological assessments include muscle wasting and examining the power and tone of the lower limbs. These assessments will indicate the chances of neuromuscular disorders on the child.
The gait condition is present when the child shows signs of out-toeing or in-toeing. In-toeing is the condition where the child’s feet points inwards rather than being flat and straight. On the other hand, out-toeing is a condition where the child’s feet curves outwards rather than flat and straight. Out-toeing is usually caused by external femoral torsion, tibial torsion and rotation of the hip contracture (Duque & Kiel, 2008).
The gait condition is mostly not complicated, and children develop the right walking patterns when they grow older. In my patient situation, I would advice his parents on the best practices, which reduce the gait abnormality. It is important for parents to understand the gait condition well. This will enable them look out for their children well. The gait abnormality does not seriously affect children. Children with in-toeing and out-toeing can walk barefooted without having difficulties with their feet. However, when the situation intensifies, this may cause the child to frequently stumble. Nevertheless, the gait abnormality does not tamper with the way children learn how to walk (Porth & Mattfin, 2008).
The gait abnormality is not complicated compared to other pathological disorders. Bow legged, and limping disorders are different from the gait disorder. If the patient shows signs of poor knee alignment and limping, they should be referred to physicians for further treatment. However, physicians can carry out a radiographic evaluation or surgery in older children, when the situation becomes complicated (Duque & Kiel, 2008).
Question 4
Candidiasis is a form of skin infection that affects people on most parts of their skin. The disease is more prevalent on the oral mucosa, skinfolds, cuticles and genitals. The signs and symptoms of the disease may vary depending on the area of the skin that is affected. The clinical presentation of the disease will determine the method of diagnosis.
Development of the disease
Cutaneous candidiasis is a type of the candidiasis infection that affects the intertrigenous areas of the body. The infection develops at individual spots in the body at it later spreads to other confluent areas in the body. In my clinical patient situation, patient education is necessary in order to prevent the patient from using the wrong anti fungal while confusing the candidiasis infection with a sexually transmitted disease.
Candida is a yeast infection that exists on the human body harmlessly. Dampness and heat create a favorable condition for the yeast to grow on the skin. Further, poor hygiene, hot weather, restrictive clothing and inflammatory diseases are the major risk factors towards the development of the infection. The disease presents itself with erythematous patches of different sizes. In addition, the disease is well demarcated and it is pruritic (Calderone, 2002).
Diagnosis for candidiasis
Diagnosis of the infection is based on the levels of potassium hydroxide amounts and the clinical appearance. Medical practitioners will determine the method of diagnosis after identifying the specific yeast causing the infection. The disease has wide levels of wet potassium hydroxide and this is diagnosed by applying drying agents. In addition, oral and topical antifungals are also possible diagnoses to reduce the spread of the candidiasis infection (Calderone, 2002).
Question 5
Tinea corporis is a fungi skin infection that is commonly known as ringworm. The fungus infection develops on various places on the human skin including the beard area, groin, scalp and between the toes. The fungi that cause tinea corporis are called dermatophytes. These fungi mostly develop on the dead tissues of the nails, hair and the surface of the skin. The disease affects people of different ages including children and adults.
Development of the disease
The fungus mostly develops on moist and warm areas of the skin. The infection mostly affects people with wet skin, minor nail and skin injuries, those with poor hygiene and it can be transmitted from one person to another. Consequently, the fungus can spread through sharing items with an infected person. These items include clothes, combs, shower floors and poor surfaces. Further, pets can spread the fungus to human beings (Patterson, 2013).
Comparison of tinea corporis and candidiasis
Tinea corporis is a fungus infection whereas candidiasis is a yeast infection. Tinea corporis is limited to the body areas with dead tissues while candidiasis affects the intertrigenous parts of the body. Ringworms are less severe than candidiasis. Ringworms exist in small patches with different shapes and sizes similar to candidiasis. However, candidiasis spreads widely to most parts of the body causing an inflammatory rash. The risk factors that cause the two infections are widely similar. For instance, poor hygiene and sharing of objects may lead to establishment of the infection. The major similarity between the two diseases is that the two infections develop in warm and moist areas of the body (Calderone, 2002).
Different types of tinea infections
There are various types of tinea fungus infections. Tinea pedis is a type of tinea fungus infection that affects the epidermal layers in the skin. Tinea pedis is an interdigital infection that mostly affects the areas between toes. The fungus infection is widely known as athlete’s foot. On the other hand, Tinea unguium affects the nails. The fungal disease is not common with children, but it establishes itself of adults who have undergone puberty and it further develops with age (Patterson, 2013).
Diagnosis of the disease
The diagnosis of tinea pedis and tinea unguium depends on the prevalence of the disease. In most diagnoses, patients who suffer from tinea pedis and tinea unguium are treated with anti fungal agents. However, tinea unguium is difficult to treat even with anti fungal agents because of the difficulties in penetrating the nail plate (Porth & Mattfin, 2009).
Question 5
Lesions are caused by multiple factors. They can be caused by human mite infestation and transmission of the infection from one patient to another. The human mite causing crusted lesions is scientifically known as sarcoptes scabiei. The predisposing factors that led to the disease infection include poverty, immunocom promised states, war refugees, crowding and closed institutions. Researches carried out on the infection reveal that the infection rate is higher where people are subjected towards the above predisposing factors (Patterson, 2013).
Relationship between primary lesions and secondary lesions
There are various categories of skin lesions; primary and secondary lesions primary. Lesions have different varying characteristics including texture and color. Environmental agents (such as temperature changes), allergic reactions (such as contact dermatitis) and infectious diseases (such as psoriasis) cause these lesions. On the other hand, secondary lesions develop because of pre existing primary lesions. Primary lesions develop in to secondary lesions because of manipulation of the lesions through scratching (Porth & Mattfin, 2009).
Types of primary lesions
Types of primary lesions include; macule, vesicle, pustule, papsule, nodule, wheal and telangiectasia. Macules include moles and freckles, which exist in different shapes and different colors. Further, vesicles are lesions that are filled with a fluid. They are raised lesions that include blisters and bullae. The cause of these lesions includes, sun burns, chemical irritation, insect bites and chemical irritation. Pustule lesions are caused by an infection. An example of a pustule lesion is a boil.
Papule lesions have a solid rough texture and they exist in different colors and shapes. These types of lesions are associated with conditions such as skin cancer. Consequently, nodule lesions resemble papule lesions but they are deeper with distinct edges. These lesions exist because of conditions such as keratinous cysts and lymphomas. Wheal lesions occur in a form of a skin elevation that are itchy. However, these lesions disappear when the lesion erupts and they are usually caused by an allergic reaction. Talengiectasia are blood vessels that are dilated and they appear close to the skin. They are usually symptoms of a developing disease such as scleroderma (Patterson, 2013).
Types of secondary lesions
Secondary lesions include; ulcers, scale, crusts, erosions, excoriation, scar, lichenification and atrophy. Ulcers affect the upper layer of the epidermis and the lower part of the dermis. They are caused by acute conditions which include; bacterial infections, chronic conditions and disorders of the peripheral veins. Scale lesions are dry and they build up from dead cells causing scales on the surface of the skin. They are caused by fungal infections such as psoriasis. Further, crusts comprise of a dried combination of serum, blood and pus. The healing of infectious lesions often causes crusts lesions. Erosion lesions cause loss of the epidermal skin layer. Consequently, excoriations are hollow and crusted. Scratching of a primary lesion leads to excoriation lesions. Scars are discolored tissues that replace the dermis after permanenet distruction. Lichenification lesions are characteristics of atopic dermatitis and dermatitis. Atrophy lesions mostly occur in the skin of individuals whose strong corticosteroid medication (Patterson, 2013).
Diagnosis of the disease
Various diseases and conditions cause skin lesions. The diagnosis for lesions is based on various conditions including the nature of the lesion, where it appears and the patient medical history. To determine the cause of the lesions, samples are taken for the lesion scrapings and they are examined in the laboratory. Dermatologists may use subdued lighting and contrast lighting to examine the skin variations (Patterson, 2013).
Clinical situation
In my medical situation, the crust lesions resulted from scratching of primary vesicular lesions. The treatment of the crust lesions will entails removal of the allergen causing the lesion from the patient’s environment. Topical preparations, such as topical creams, solutions and lotions, are used to clean up the irritated skin. Oral medication is also necessary to eliminate systemic conditions or infections.
References
Porth, C.M., & Matfin, G. (2009) Pathophysiology: Concepts of altered health states. (Eight ed.) Philadelphia, PA
Patterson, J. W. (2013). Practical skin pathology: A diagnostic approach. Philadelphia, PA: Elsevier/Saunders.
Sussman, C., & Bates-Jensen, B. M. (2007). Wound care: A collaborative practice manual. Philadelphia: Wolters Kluwer Health / Lippincott Williams & Wilkins.
Calderone, R. A. (2002). Candida and candidiasis. Washington: American society of microbiology.
Duque, G., & Kiel, D. P. (2008). Osteoporosis in older persons: Pathophysiology and therapeutic approach. London: Springer.
Hamdy, R. C., & Lewiecki, E. M. (2013). Osteoporosis. New York: Oxford University Press.
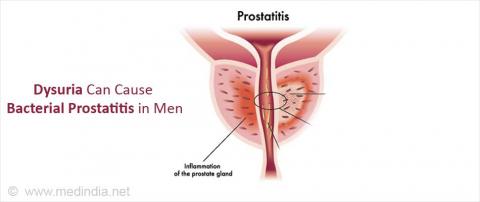 Dysuria is irritating, painful, uncomfortable and sometimes burning when it has progressed. There are multiple causes of the infection. However, urinary tract diseases are the most frequent causes of the infection. The disease can affect various parts of the urinary tract such as ureter, bladder, kidneys and the urethra. The infection is mostly caused by bacterial pathogens, which enter the urinary tract via the urethra.
Dysuria is irritating, painful, uncomfortable and sometimes burning when it has progressed. There are multiple causes of the infection. However, urinary tract diseases are the most frequent causes of the infection. The disease can affect various parts of the urinary tract such as ureter, bladder, kidneys and the urethra. The infection is mostly caused by bacterial pathogens, which enter the urinary tract via the urethra.
The thesis of essay is to analyze the physical examinations, laboratory tests and treatment plan that would be carried on a 51-year-old female patient who has dysuria. This essay will focus on the right diagnosis tests that are likely to be performed on the patient, with evidence pertaining the relevance of the diagnoses.
The patient explains that she has experienced lower abdominal pains, nausea without vomiting and high temperatures of about 100 degrees. There are various causes of dysuria, and they reflect in the physical examinations and urinalysis tests. Thus, it is vital carrying out physical examinations, urinalysis and lab tests to establish the cause of the infection.
The first step in diagnosis would be examining the patient’s past medical history. This brings out the possible causes of the disease condition. Further, physical therapy is important to establish the condition of the abdomen, external genitalia. The examination of the external and internal genitalia organs will help evaluate the degree of infection and the cause (Ferri, 2012).
The physical therapy required will evaluate the chances of infection or non-infection causes of the dysuria. Dysuria is sometimes caused by the conditions of the external and external genitalia conditions of the patient. Most dysuria infection is caused by a reduction of the endogenous estrogen, which in turn lead to the disease condition. Further, if the vaginal epithelium occasionally experiences inflammation and dryness, this may lead to dysuria (Buttarp, Trybulski, Polgar & Sandberg-cook, 2013).
Therefore, in order to examine the condition of the dysuria, I would enquire for a cystoscopy examination. Cystoscopy examinations reveals the conditions of the internal genitalia organs. The procedure is digitalized and the results are portrayed on a digital screen. Thus, the report is accurate (Ferri, 2012).
Consequently, the dysuria condition may result from various bacterial infections. For instance, it may result from cystitis, pyelonephritis, urethritis and vaginitis. Thus, in order to establish the pathogenic cause of the infection the medical practitioner should order for a urine test in the laboratory. Consequently, the other symptoms present in the patient’s condition such as nausea and fever, the medical practitioner should order for a blood test. Blood tests are vital in evaluating the cause of the fever and if there are pathogens present in the blood. The test examinations will reveal the bacterial cause of the infection, and it will determine the most ideal medication prescription for the patient (Ajithkumar, 2011).
Patient treatment plan
The treatment plan for the dysuria patient should incorporate wide aspects of drug treatment, and urinary retention therapy. Consequently, the medical practitioner would consider collaborating with various professionals such as physicians to manage the abdominal pain. Further, follow-up measures should be set up after the patient discharge to ensure the effectiveness of the patient and to avoid the condition from occurring again in the future.
Urinary retention therapy
After establishing the cause of the dysuria condition, the medical practitioner should consider engaging the patient in a urinary retention therapy to repair the tissue damage caused by the infection. For instance, renal impairment may be cause renal tissue damage. Thus, after establishing the disease, the medical practitioner should carry out a tissue repair treatment on the patient. Urinary therapy mainly focuses on ensuring the patient resumes the right flow-rate and urinal frequency (Ajithkumar, 2012).
Drug therapy
Consequently, another cause of the abdominal pain may be the occurrence of dysmenorrhea. It should not be ruled out since the female patient has is old enough to experience menses. Dysmenorrhea is simply painful menstruation (Buttarp, Trybulski, Polgar, Sandberg-cook, 2013). Dysmenorrhea may be caused by production of too many prostaglandins that may cause contraction of the myometrium which in turn may result in pain (Golan & Tashjian, 2012). The most likely dysmenorrhea expected would be primary dysmenorrhea. The management of this condition would involve the use of non-steroidal anti-inflammatory drugs. The drugs include Ibuprofen, Meclofenamate or Naproxen (Ferri, 2012).
Further, the medical practitioners should asses the conditions leading to the painful urination. These can be achieved by establishing the cause of the infection and disinfecting it. Consequently, if the condition is caused by an organ malfunction, then the physiotherapy would be vital for the patient.
Preventing the risk factors
The risk factors causing dysuria condition include pregnancy, diabetes, obesity, abnormal bladder function and kidney stones. The treatment plan should aim at reducing the prevalence of the risk factors through patient education. This will enable the patient learn the predisposing factors leading to the condition and how to reduce the level of the predisposing factors. For instance, the patient should consider taking regular exercises, regular check-ups, eating healthy and taking more fluids during recovery to improve the dehydration condition caused by frequent urination (Buttarp, Trybulski, Polgar, Sandberg-cook, 2013).
References
Buttarp, M., Trybulski,J., Polgar, B, P., Sandberg-cook, J., (2013). Primary Care. Elsevier Health Science Division ISBN: 9780323075015.
Ferri, F. F. (2012). Ferri's clinical advisor 2013: 5 books in 1. St. Louis, Mo: Elsevier Mosby.
Ajithkumar, T. V. (2011). Oxford desk reference. Oxford: Oxford University Press.
What other toxicities occur with neuromuscular junction blocker administration?
 Succinylcholine stimulates nicotinic and muscarinic receptors. This cause various unwanted side effects that limits its use in clinical practice. For instance, succinylcholine causes stimulation of muscarinic receptors located in the sino-atrial node that produces bradycardia. This mostly occurs in patients with high vagal tones especially children (Claus, 2012).
Succinylcholine stimulates nicotinic and muscarinic receptors. This cause various unwanted side effects that limits its use in clinical practice. For instance, succinylcholine causes stimulation of muscarinic receptors located in the sino-atrial node that produces bradycardia. This mostly occurs in patients with high vagal tones especially children (Claus, 2012).
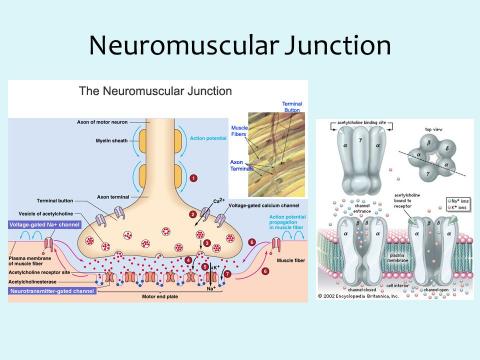
What is the pharmacologic effect in skeletal muscle following neuromuscular junction blocker administration?
Neuromuscular junction blockers are administered through IV. They make the skeletal muscles flaccid and nonreactive to neuronal stimulation. Small muscles that cause rapid movement, such as muscles present in the eyes, become paralyzed faster than other larger muscles located in the neck and head. Further, the muscles in the other parts of the body such as limbs are paralyzed after some time. The diaphragm is the last to be affected by administration of these drugs and respiration ceases. However, with careful monitoring of patients, the adverse effects can be controlled (Clauss, 2012).
What are the pharmacologic effects of epinephrine and norepinephrine?
Norepinephrine produces an intense venous and arterial vasoconstriction in all the vascular beds. Further, it lacks bronchodilating effects on the airway smooth muscles. Norepinephrine rarely causes hyperglycemia. Moreover, a continuous norepinephrine infusion can be used to diagnose refractory hypotension. Norepinephrine IV administration causes intense vasoconstriction in the liver, skin, kidneys and vasculature of skeletal muscles. This leads to increased systolic, mean arterial and diastolic pressure (Strauss, 2013).
Are there any special considerations in the administration of catecholamines to pediatric and geriatric patients?
Both geriatric and pediatric patients should be put under close monitoring to prevent manifestation of the unwanted adverse effects of these drugs. In pediatric patients, the blood-brain barriers may not be fully developed. Thus, harmful drugs may lead to toxicities in the brain (Strauss, 2013).
References
Clark, M. A. (2012). Lippincott's illustrated reviews. Baltimore, MD: Wolters Kluwer Health/Lippincott Williams & Wilkins.
Strauss, H. W. (2013). Nuclear oncology: Pathophysiology and clinical applications. New York: Springer.
Browse More Essay Topics 24/7/365 Support 11+ Yrs in Essay Writing Pay for Quality not Quantity Score that A+ Grade